Description of ACL Injuries
The anterior cruciate ligament, or ACL, is one of four major ligaments that make up the knee. Ligaments are in place to stabilize the femur (thigh bone), which sits just above the tibia (shin bone).
The ACL is critical to maintaining knee stability. ACL injuries are very common among athletes of all ages and competitive levels. Approximately 200,000 ACL injuries are reported each year in the United States. Soccer, football, skiing, lacrosse and basketball are some common examples of higher-risk sports that see a high number of ACL injuries. In almost all sports, the rate of ACL tears is higher in women than in men.
Normal Intact ACL

Sagittal MRI scan demonstrating the normal ACL. The ACL courses from the posterior aspect of the femur, close to the articular cartilage margin posteriorly, to the tibia essentially directly in line with the anterior root attachment of the lateral meniscus. .
CLICK IMAGE TO ENLARGE
Mid-Substance ACL Tear
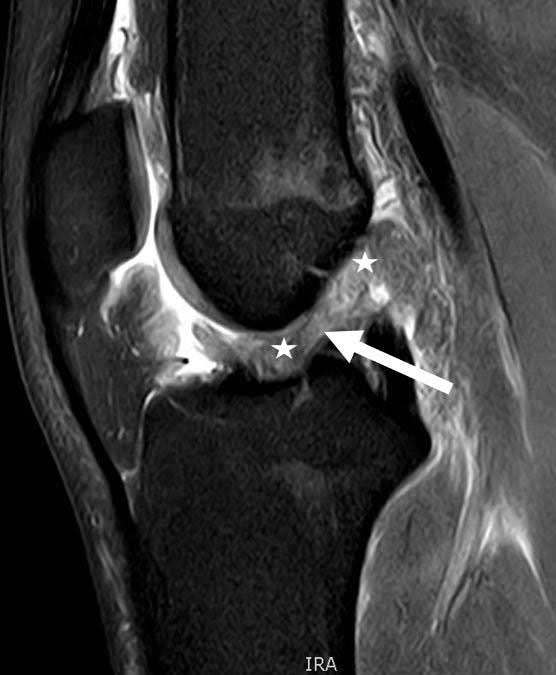
Sagittal MRI scan demonstrating a mid-substance tear of the ACL. There is a loss of continuity of the normal fibers, indicating the ACL is torn.
CLICK IMAGE TO ENLARGE
Symptoms of an ACL Injury:
- Patients with an ACL tear often report instability in the knee and a
- Feeling as if it will “give out”, or pop out of place
More times than not, patients will opt to have ACL surgery to treat the injury because of the desire to resume contact or twisting sports, such as skiing. A large majority of ACL injuries—approximately 50 percent—occur in combination with an additional injury and damage to the meniscus, articular cartilage, or other ligaments.
In addition to role in providing stability, the ACL also provides protection for the menisci of the knee. When the knee continues to have instability episodes, it is not uncommon for the medial or lateral meniscus to tear. However, with the presence of a meniscal tear there is much higher risk of developing osteoarthritis. Because of this, Dr. LaPrade usually recommends ACL reconstruction for an ACL tear in young or otherwise active patients, in patients who have meniscal tears, and in almost all patients who report instability with twisting or turning activities.
Dr. LaPrade will evaluate the patient’s knee to determine if in fact an ACL tear has occurred through a series of clinical tests, x-rays and an MRI. The MRI will also determine if there is an injury associated with another knee ligament, the meniscus or articular cartilage.
In order to verify if the ACL is in fact still intact, Dr. LaPrade will perform the Lachman’s test. In a torn ACL, increased forward movement will be felt in relation to the tibia and femur. This will feel mushy and soft which is the result of an ACL tear. Other tests may also be used including the Pivot Shift Test to check for anterolateral instability of the knee.
Degrees of an ACL Injury:
- Grade I Injury: A Grade I injury of the ACL does not involve a tear, but instead, minor stretching of the ligament which may show up as swelling in the ligament on MRI. Patients will feel swelling and tenderness but will be able to resume normal activities for the most part.
- Grade II Injury: This injury represents a partially torn ACL (usually one of the two bundles) and is considered to be more serious. Inflammation will occur and soreness to the knee will be present. Walking for patients is usually more difficult. Surgery may be recommended.
- Grade III Injury: This injury occurs when the ACL is torn completely. Patients are usually in severe pain; inflammation and swelling will peak and walking without a limp will become difficult if not impossible.
Have you sustained an ACL injury?
There are two ways to initiate a consultation with Dr. LaPrade:
You can provide current X-rays and/or MRIs for a clinical case review with Dr. LaPrade.
You can schedule an office consultation with Dr. LaPrade.
(Please keep reading below for more information on this condition.)
How to Read a MRI of an ACL Tear
Treatment for an ACL Tear
For patients who experience a Grade II or Grade III ACL tear and who have a meniscus tear, there is a much higher risk for the development of osteoarthritis in the future. Because of this, Dr. LaPrade will usually recommend a combined meniscus repair and ACL reconstruction to be performed, and for ACL reconstructions to be performed in young or otherwise active patients and in almost all patients who report instability with twisting or turning activities.
The technique of ACL surgery has changed dramatically over the last decade in the orthopaedic (orthopedic) community. Anterior cruciate reconstruction grafts performed prior to 5-10 years ago were placed more centrally on both the tibia and femur – research has shown many of these patients have continued problems with rotation instability. This problem became recognized through extensive clinical and biomechanical research and the surgical technique has changed to where the reconstruction tunnels are now placed more anatomically to provide better stability to the knee. Dr. LaPrade’s research team has been instrumental in helping better define the anatomy that has lead to improved ACL reconstruction techniques.
Post-Op
It is absolutely essential for a well-supervised physical therapy protocol following ACL reconstruction surgery. Reactivation of the quadriceps mechanism, edema control, patella mobilization, maintenance of full knee extension and regaining knee motion are absolutely essential to obtaining optimal post-operative outcomes. Dr. LaPrade strongly suggests and requires patients to remain in Vail, Colorado to work with our physical therapists at Howard Head Sports Medicine for a minimum of 5-7 days post-operatively to ensure they are having proper care post-operatively and also so that their rehabilitation will advance to high levels at a quicker pace.
Related Studies
- Biomechanical Comparsion of Anatomical Single and Double Bundle ACL Reconstruction
- Functional ACL Bracing – Current State
- Femoral Cortical Suspension Devices for Soft Tissue ACL Reconstruction
- Biomechanical Comparison of Tibial Fixation for Soft Tissue ACL Grafts on the Tibia
- Effects of Grade III PLC Injuries on ACL Grafts
ACL Injury FAQ
1. What does an ACL tear feel like?
An ACL tear can feel different depending upon the mechanism that caused the tear and the type of sport that an athlete is participating in. About 70% of ACL tears are noncontact. In these tears, an athlete will commonly be twisting and turning when their ACL will tear. Also, about 70-75% of the time a patient who tears their ACL will feel a pop. This pop is believed to be due to a bone bruise which is caused when the outer part of the knee slips upon itself and bruises the front part of the femur and the back part of the tibia. In general, people who have only torn their ACL, that is they do not have a meniscus tear or other ligament tear, do not have problems walking straight ahead and usually have problems with twisting, turning, and pivoting. People who have torn their ACL who have problems with straight-ahead activities may have other injuries in their knee that is contributing to that problem.

Sagittal MRI scan demonstrating a typical bone bruise pattern of the lateral compartment associated with an ACL tear. The bone bruise on the back portion of the outer port of the knee and the lateral tibial plateau essentially hit against the front part of the femur on the lateral femoral condyle. These two bone bruises indicate the amount of subluxation that occurred on the outer part of the knee with an ACL tear. Due to this amount of movement, it places the lateral meniscus at risk, especially the lateral meniscus root, for a tear. About 70% of ACL tears have this bone bruise pattern. This bone bruise pattern is also felt to be the cause of the pop that patients sometimes feel when they tear their ACL.
CLICK IMAGE TO ENLARGE
2. Why do ACL tears happen?
ACL tears usually happen because the knee is put a biomechanically disadvantaged position and the ACL is not able to withstand the forces placed on it. This can be due to muscle fatigue, bad mechanics, or a lack of proprioception by an athlete. In very high level sports, the margin of error between being able to catch ones knee and not have an injury and sustaining an ACL tear can be minimal. In patients who may be deconditioned, or have poor mechanics, the ACL can be put at a more disadvantaged position much more easily during these circumstances.
3. Why are ACL tears common?
ACL tears are one of the most common knee ligament injuries. The most common knee ligament injury is the MCL, which often tears and is able to heal on its own when it is isolated. However, in general, most ACL tears do not heal and require surgery. It is estimated that over 350,000 ACL reconstructions were performed in the U.S. last year. Thus, it is the commonly performed knee ligament surgery. The number of ACL tears seems has increased as the number of participants in sports has increased. This is especially in women athletes, with women’s soccer, women’s basketball, and women’s volleyball being very high risk sports for ACL tears.
4. Why does an ACL not heal?
An ACL tear does not heal because it does not have a good blood supply and it is located in the harsh intraarticular environment of the knee. The normal knee joint lining secretes enzymes which dissolve blood. This is beneficial to the knee itself so that it does not form a big blood clot inside the knee when one does have bleeding and the blood can be more easily resorbed over time. However, a blood clot is necessary for a ligament to heal. Thus, because of the enzymes that are created (plasmin) blood clots almost never form within the knee and this does not give the ACL a good chance to heal.
5. How does an ACL work?
The anterior cruciate ligament is the main stabilizer to the knee in preventing the tibia from sliding forward on the femur. It is most effective as a knee stabilizer with the knee at about 20-30 degrees of knee flexion and this is where clinicians will generally check a knee to determine if the knee slips forward, which would be consistent with an ACL tear and clinical exam (the Lachman test). The ACL is also important to knee stability to ensure that the tibia does not internally rotate on the femur. This is a shifting that can occur when one has an ACL tear when they plant their foot, twist and turn, or pivot, and the knee can partially dislocate (sublux). This is the most disabling portion of an ACL tear.